
General examination
Avoid the tendency to examine only the feet. Check the spine, upper limbs for evidence of neurological disease or arthritis, proximal limb alignment and joints. Foot and ankle surgeons need to be amateur neurologists!


This lady was referred with progressing claw toes. She had asymmetric cavus feet, which tends to suggest spinal problems. She had a hairy patch, spina bifida and diastematomyelia
Look
Look at shoes and orthoses

Look at the patient's shoes - could this foot fit in this shoe? Frey found that American women wore shoes 1cm narrower than their shoes. Same in Blackburn!

We ask patients to bring all orthotics with them - it give you an idea what has been tried and what modifications might be made. Sometimes orthotics are fine but don't fit.
Look at the feet
- pes cavus associated with claw toes, suggesting an underlying neurological condition
- other evidence of rheumatoid disease
- hallux valgus or other first ray problems, which may shift loading laterally
- submetatarsal calluses, indicating high loading, possibly because of the plunger effect
- pressure points or soft corns between the toes

Sub-metatarsal calluses indicate areas of pressure and shear

Soft corn - very small, very painful
Feel
Feel for tenderness over deformities, around metatarsal heads and MTP joints.

Distinguish between tenderness under the MT head (orange), suggesting pressure, and under the MT joint (red) suggesting instability and/or synovitis
Move
Measure active and passive ranges of movement of all the joints
Check for:
- restricted movement
- contractures
- simulation of pain by movement
Details of assessment of deformity and movement of a hammer second toe.
There is a hyperextension deformity of the MTP joint and a flexion deformity of the PIP joint.
In this case the DIP joint is straight - in some hammertoes it is extended.
Neither the MTP or PIP joint deformities can be passively corrected with the toe relaxed. In Blackburn we would class this as a type 3 toe:
- Type 1 - PIP joint reducible flexion, MTP joint reducible hyperextension
- Type 2 (the commonest) - PIP joint fixed flexion, MTP joint reducible hyperextension
- Type 3 - PIP joint fixed flexion, MTP joint fixed hyperextension or dislocation
Check the stability of the MTP joint using the Thompson-Hamilton draw test.
Hold the metatarsal in one hand and the proximal phalanx of the toe in the other. Thompson and Hamilton performed the test with the toe in neutral dorsiflexion/plantarflexion; we find slight plantarflexion helpful if the long flexor tendon is tight.
The toe is translated vertically with a technique like that of the Lachmann test in the knee. Sometimes there is no instability but the patient's pain is reproduced. Vertical translation can be felt and subjectively graded as:
- Grade 0 - no translation
- Grade 1 - less than 50% translation
- Grade 2 - 50-100% translation
- Grade 3 - dislocatable
Clinic tests
Do a full neurological examination, including protective sensation testing with Semmes-Weinstein filaments. Feel pedal pulses, assess capillary circulation and do Doppler blood pressure measurements if necessary
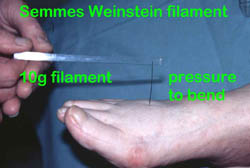
Do a relevant neurological examination, including measurement of protective sensation with Semmes-Weinstein neurofilaments

Check peripheral circulation, including Doppler pressures where indicated