
Plain radiography is not usually very helpful. Oblique views of an acutely injured ankle may show an avulsion fragment lying lateral to the lateral malleolus – this represents a flake of bone avulsed with the SPR.
Both ultrasound and MR can show the tendons well and demonstrate tears. Both modalities can assess the ankle ligaments. MR also enables assessment of the depth of the peroneal groove and will demonstrate intra-articular problems in the ankle such as osteochondral injuries. Tendonopathy shows as enlargement, high signal or a “flame” shape to the tendon. Tears show as multipart or chevron-shaped tendons, and part or all of the tendon may be subluxed laterally. Small studies in comparison with surgery suggest high sensitivity but specificity is difficult to assess as normal patients were generally not operated on.
Grant et al (2005) reported ultrasonography in 58 patients, 30 of whom were surgically explored. Ultrasound had a sensitivity of 100% and a specificity for differentiating tears from other appearances, but again most patients with ultrasonographically normal tendons were not explored and their clinical outcome was not reported. Grant et al commented that the most difficult diagnosis on ultrasound was to identify a peroneal tear in the presence of chronic tenosynovitis, when it is difficult to distinguish between the tendon and the thickened paratenon.
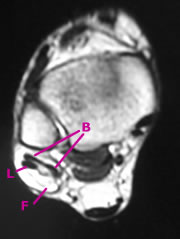
Transverse MRI - partial peroneus brevis tear
B - brevis (note broad thin tendon with central split
L - longus
F - fluid and synovitis in paratenon
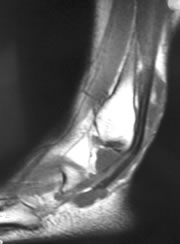
Sagittal MRI - partial peroneus brevis tear
Thinned brevis, longitudinal high signal in longus suggesting tear
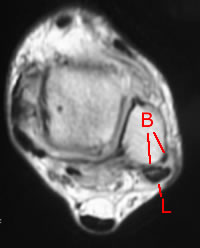
MRI - peroneal tendon subluxation with type 2 instability
B - brevis (note two strands of torn brevis tendon)
L - longus