
Plain radiographs
The traditional plain radiographs are a lateral hindfoot view and an axial view of the calcaneum. Utukuri et al (2000) showed that the axial view contributes little to the diagnosis of fracture, and CT will be required if surgery is planned. Therefore, as it painful for the patient to obtain an axial view and it represents a radiation dosage, we do not routinely use this view in the emergency department. It is useful intra-operatively to show reduction of the body and medial wall fragments.

Fracture of the tuberosity
Extra-articular body fracture

Posterior avulsion fracture pulled off by the Achilles tendon
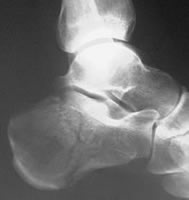
The lateral view not only allows the diagnosis of a body or peripheral fracture to be made with confidence in most cases, but with careful analysis will give useful information about damage and displacement of the subtalar joint. Indeed, Ebraheim (1996) has shown that the plain lateral view will give additional information on subtalar fragment displacement compared with CT in 25% of patients, and Ogawa (2009) found that CT consistently underestimated the posterior facet depression compared with the plain lateral view.
Bohler's angle
The crucial angle of Gissane
On the lateral view, the principal landmarks are:
- the subtalar articular facet – multiple shadows indicate fragments and their displacement
- the angle of Bohler – normal value 25-40 deg, may be reduced to a negative value in a highly-impacted fracture and this has prognostic and treatment-planning significance
- the crucial angle of Gissane between the subtalar facet and the anterior surface – this angle needs to be reconstructed if surgery is performed

Lateral view

The posterior facet should be here...

...but it has rotated downward to here
Tomography
May be used if CT is unavailable but may fail to show joint incongruity adequately.
Broden’s views
AP views with leg internally rotated 30°. Films are taken with tube angled 10°, 20°, 30°, 40° toward head.Broden views show the joint surface well, but probably underestimate displacement compared with CT. They require expertise on the part of the radiographer. Although CT is preferable, they may be useful if this is not available, and are useful intra-operatively to assess reduction of the subtalar facet, and post-operatively to assess maintenance of reduction.

Coronal CT of a type 2B fracture
CT
CT should now be considered the gold standard for assessment of intra-articular os calcis fractures. It gives excellent images of subtalar joint surfaces, degree of displacement (Janzen et al 1992) and soft tissue injuries (Bradley and Davies 1992). It may not be so good for imaging the calcaneocuboid joint. Imaging of the subtalar joint is superior to plain films (Janzen et al 1992); no study that I can find has compared Broden views with CT. However, the plain lateral view will cantribute additional information in 25% of patients (Ebraheim 1996), and Ogawa (2009) found that coronal CT tended to underestimate joint depression compared with the plain lateral radiograph. Sagittal reconstruction was not used in Ogawa's study, although this is usually available from modern scanners.
Both feet should be scanned, with image acquisition in both coronal and axial planes. The CT gantry is inclined to be at right angles to the subtalar joint surface. 3-D reconstructions may be performed, although their value is debatable.
MR
MR has been described in the assessment of calcaneal fractures. It gives excellent imaging of soft tissue injuries, especially to the peroneal tendons. However, CT usually gives superior imaging of bone and no study has shown that MR adds important information in the typical patient.