
Chondral and osteochondral lesions or defects are an important source of pain after ankle injuries. The advent of CT and MR scanning has shown that they are commoner and more complex than was thought.
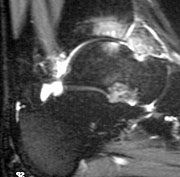
MRI scan - osteochondral lesion on the talus with "kissing" lesion on the plafond
Although the majority of osteochondral lesions occur after a definite injury, some have no clear history of injury. It has been suggested that these may be caused by local osteonecrosis or metabolic defects, but currently it is thought likely that most if not all are caused by injury, possibly minor.
Most OCDs occur on the talus, but about 10% occur on the tibial plafond, often as “kissing lesions” with a talar defect. Talar lesions usually occur in two distinct regions:
- medially
- 70% of talar lesions
- 50-70% have a history of injury
- tend to be deep and “cup-shaped”, and may be cystic
- laterally
- 30% of talar lesions
- almost all have a history of injury, usually inversion ± dorsiflexion
- usually more superficial and “wafer"-shaped
- more likely to displace
It is often said that medial lesions tend to be posteromedial, and lateral lesions anterolateral. However, a series of over 400 lesions reported by Raikin (2007) found that the majority of lesions on both sides of the talus were in the central third of that side.
Berndt and Hardy (1959) suggested that lateral lesions are caused principally by shear and twist, accounting for the wafer-shaped lesions; while medial lesions were caused by impaction with a plantar-flexed ankle. In cadaver studies they could reprodice typical lesions. However, patients with medial lesions often do not have nay clear history of such an impact.
A useful review is O'Loughlin (2010) - American Journal of Sports Medicine 38:392-404