
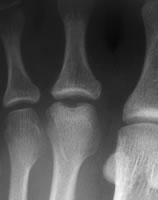
Freiberg's disease of the second metatarsal head - the commonest site
Freiberg's disease is an "infraction" of the dorsal part of one of the lesser metatarsal heads. Gauthier and Elbaz (1979) recorded 2/3 of lesions in the second metatarsal, 1/4 in the third, 4% in the fourth and only one in the fifth. There is a partial collapse of the metatarsal head, with degenerative change in the joint. The lower part of the head, however, is normally well preserved. Gauthier and Elbaz described five stages (with the number of cases in their series):
- stage 0 - subchondral fracture (1 case)
- stage 1 - osteonecrosis without deformation (6 cases)
- stage 2 - deformation by crushing of the osteonecrotic segment (26 cases)
- stage 3 - catilaginous tearing (26 cases)
- stage 4 - arthrosis (29 cases)
Several papers attribute a similar classification to Smillie (1957) but this reference is an abstract which does not, in itself, contain a classification.
Freiberg's is a condition of young adults. Some series report about half have a clear history of trauma and others of repeated stress. Stanley (1990), however, found only a weak relationship with trauma, repeated stress and wearing high-heeled shoes, but found the affected metatarsal long in comparison with the adjacent rays in 85% of 31 feet.
A useful review of Freiberg's disease was produced by Carmont (2009).
Clinical features
Most patients complain of pain in the affected joint, usually quite clearly localised in the upper or lower part of the joint, but sometimes more generalised across the forefoot, and may simply be referred as "metatarsalgia". Some patients complain of stiffness in the joint, or of osteophytes rubbing on the shoe.
The foot is usually of neutral shape. The affected joint is usually thickened and there may be tender osteophytes. The joint is stiff and manipulation reproduces the patient's pain.
Management
Many patients require only explanation of the condition and simple advice about pain control and shoe choice. Large osteophytes may make it difficult to find comfortable shoes, and pain under the affected metatarsal, or in transfer lesions, can be helped with a metatarsal dome insole; the orthotist's advice and help are valuable. The symptoms are often non-progressive, and the patient need not have any intervention simply to prevent future trouble. For more troublesome joints, an injection of steroid + local anaesthetic can help resolve symptoms.
Surgery can be offered for intractable pain or pressure symptoms. Options include:
- debridement with excision of osteophytes (Helal and Gibb 1987)
- debridement with dorsiflexion osteotomy. Gauthier and Elbaz (1979) described this in 53 patients. At an average of 22 months post-op only one patient had pain, but more specific outcom measures were not reported. Kinnard and Lirette (1991) performed the procedure slightly more proximally and reported pain relief in all 13 patients with occasional pain during jogging in 3. Chao (1999) also perfomed the osteotomy at metatarsal neck level and fixed it with pins, reporting 4 patients with AOFAS lesser metatarsal scores above 90/100, 7 at 80-89/100, and two with persistent pain and scores <80/100. Lee (2007) reported 12 patients with osteotomies fixed with PDS pins. Mean VAS pain score improved from 8.0 to 2.3/10 and MTP joint range of movement improved by a mean of 26deg. Remodelling occured in most joints. There was one delayed union with persistent swelling and the only dissatisfied patient.
- elevation of the fragment and grafting (Smillie 1957, no results quoted)
- excision arthroplasty, usually excision of the phalangeal base (an arthroscopic technique has been describe by Carro (2002)), although there are references to metatarsal head excision in some papers without results being quoted
- osteochondral plug transfer (Hayashi 2002)
- metatarsal shortening osteotomy. Duckworth (1991) simply shortened the metatarsal by 4mm through the neck without exposing the joint. The osteotomy was fixed with a mini-fragment T-plate. 15/16 patients were relieved of pain and most of the joint became more congruent. However, 7/16 joints were stiff, four toes did not touch the ground and there was one wound sinus.
- joint replacement (Bordelon 1977)